45 year old male patient with swelling over legs and abdomen and lower back pain and renal failure
This is online E-blog, to discuss our patient de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
This E-blog also reflects my patient's centred online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.











 Ascitic fluid LDH:
Ascitic fluid LDH:

 Renal function test on 2/09/2021:
Renal function test on 2/09/2021:








 4
4
 5
5




 On 01/09/2021 :
On 01/09/2021 :



On 06/09/2021:
On 01/09/2021:
 Hemoglobin:
Hemoglobin:

 On 04/09/2021:
On 04/09/2021:
 On 18/09/2021:
On 18/09/2021:


 03/09/2021:
03/09/2021:
 04/09/2021:
04/09/2021:




Following is the view of my case
CASE:
A 45 year old male patient with swelling over legs and abdomen since 3 months and back pain since 1 month
HISTORY OF PRESENTIMG ILLNESS
•Pt was apparantly asymptomatic 13 years back then he had episode of loss of consciousness with biting of tongue,no sweating , no rolling of eyes and brought to hospital and diagnosed as hyperglycemia and there after he started on insulin continued for 1 year twice daily then he stopped when blood sugar levels became normal and then after he had regular check up
• 3 months back he noticed swelling of legs which was inscidious in onset and gradually progressive , for which he went to local doctor and took medication for 4 days then he developed swelling all over body( hands, legs, scrotum, abdomen , face) and had mild shortness of breath for which he consulted our hospital and diagnosed as renal failure and started therapeutic trail with diuretic infusion and kept on hemodialysis on regular basis, not associated with loss of appetite, fever, vomiting, abdomen pain , decreased frequency of urination , burning micturition, hematuria urgency, difficulty in passing urine
• 3 months back diagnosed with hypertension and put on medication there after
•1 month back lower back pain which was sudden in onset and gradually progressive in nature which was throbbing type and non radiating , diffuse type and patient is not able to sit , getting up from chair and not able to sit cross legged , present through out the day, no relieving factors , aggaravated by sitting standing, not associated with fever, trauma
• Abdomen distension since 3 months and when distension increases, there will be increase in back pain
• 1/09/2021 therapeutic ascitic tap was done and nearly 500- 600 ml was drained which was pinkish red in colour and sent for microbiology, pathological, biochemical investigations was done
• Recent dialysis 4/09/2021, 4 pm
• Taken orthopedic consultation on 4/ 09/2021
and their provisional diagnosis was RENAL OSTEODYSTROPHY and suggested T.ULTRACET and T.PAN
History of past illness:
Known case of diabetes since 13 years
known case of hypertension since 3 months, Not a known case of asthma,epilepsy,etc;.
Had Blood transfusions 5 times
PERSONAL HISTORY
Diet- mixed
Appetite - normal
Bowel and bladder movements - decreased urination since starting of dialysis
Sleep - not adequate due to pain
Addictions/Habits- stopped consuming alcohol since 1 year before he used to consume quarter occasionally, smokes beedi stopped since 3-4 months
FAMILY HISTORY
Not significant
GENERAL EXAMINATION
Patient is conscious, coherent and cooperative and well oreinted to time place and person
He is moderately built and moderately nourished
Pallor :absent
Icterus:absent
Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Edema: present
VITALS ( on the day of admission):
On 31/08/2021:
BP - 150/90mm Hg
PR- 98 BPM
RR- 24 cpm
SpO2- 97%
GRBS-120mg%
Later on 01/09/2021
SYSTEMIC EXAMINATION:
•CVS - S1,S2 heard no murmers
•Respiratory system- vesicular breath sounds heard
•Abdomen- distended, - umbilicus everted, no visible scars , sinuses, is seen, no visible pulsation seen
Fluid thrill- positive
Shifting dullness-
•CNS- intact
Investigations:
On 31/08/2021:
Serum Iron
Serum electrolytes
Serum creatinine
Blood urea
Ultrasound scanning
Blood grouping
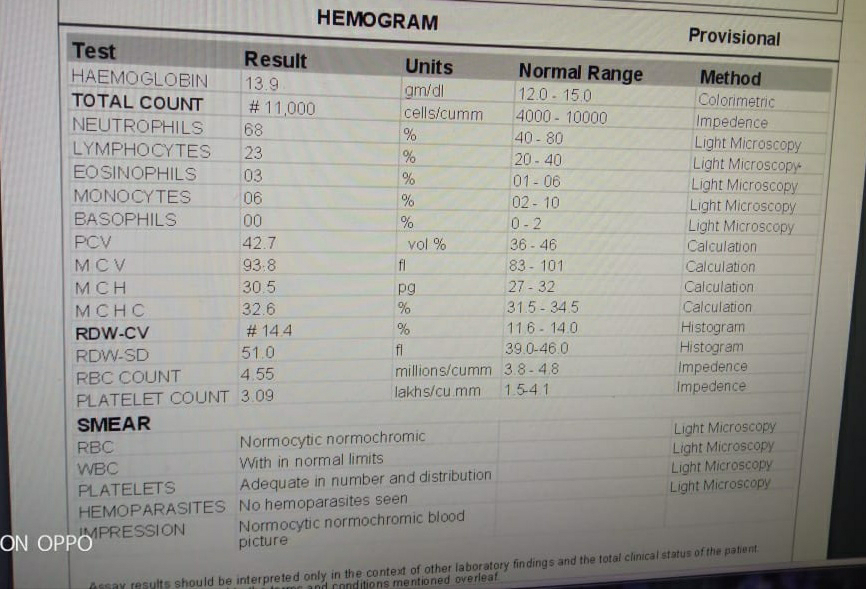
Complete blood picture
Anti HCV antibodies
HIV test
HBs Ag test
ECG
On 01/09/2021:
Ascitic fluid Sugar Protein:
Ascitic fluid Amylase:
SAAG:
As SAAG is greater than 1.1 it indicates transudate
Bacterial Culture & Sensitivity Report:
ESR:
On 02/09/2021:
Colour Doppler 2D ECHO:
X rays:
1
2
3
Inspection of the abdomen:
From Right side:
From left side:
From front side:
Pitting type of edema is seen near ankle:
On 01/09/2021 :On doing Therapeutic Ascitic tap : ascitic fluid mixed with blood is seen and around 500-600 mL of fluid is drained
On 06/09/2021:
Again Therapeutic Ascitic tap was done and around 700 mL of fluid was drained
It was also sent for analysis :
And the Hb is 2 gm /dL when they did it manually
On 06/09/2021:
Patient got blood transfusion as his Hemoglobin is low
On 08/09/2021:
Diagnostic Ascitic tap was done and sent for analysis:
PCV:
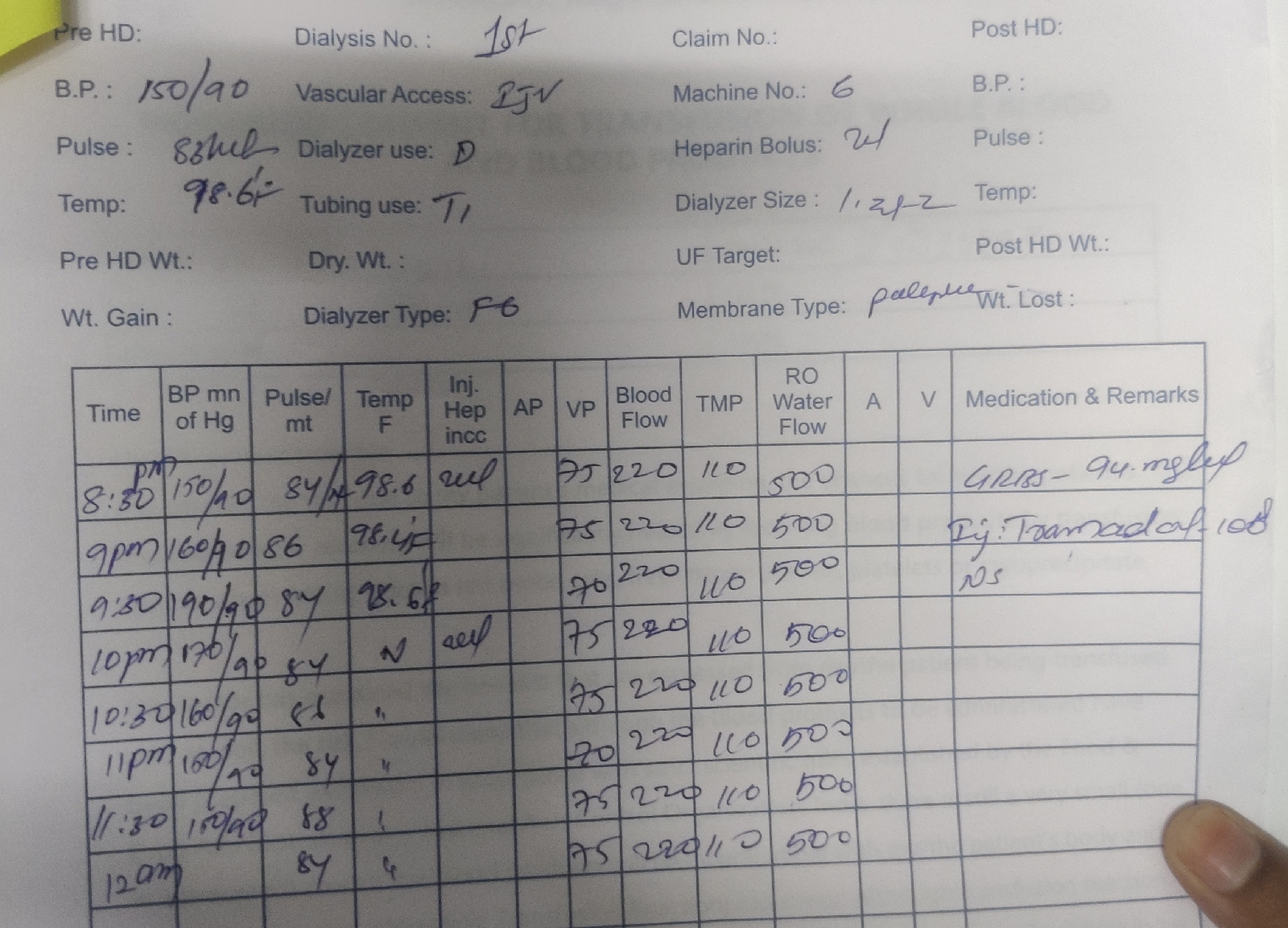
Dialysis :
On 01/09/2021:
MRI SCANNING:
*:

PROVISIONAL DIAGNOSIS
• CKD ON MHD with known case of HYPERTENSION
FOR BACK PAIN:
Renal osteodystrophy
Treatment Regimen:
1.Tab LASIX 40mg BD
(1-x-1)
2.Tab NICARDIA 20 mg BD
(1-x-1)
3.Tab OROFER XT BD
(1-x-1)
4.Tab NODOSIS 500 mg BD
(1-x-1)
5.Tab SHELCAL 500 mg OD
(x-1-x)
6.Inj ERYTHOPOIETIN 4000 IU sc weekly once
7.Inj IRON SUCROSE 1amp in 100mL NS/IV weekly once
Advice to the patient:
Salt Restriction and Restriction of Water intake not more than 1 litre per day
02/09/2021:
On 06/09/2021:
On 07/09/2021:
On 08/09/2021:
Questions:
1)Why there is blood in ascitic fluid
2)What is the cause of anemia in this patient
3)What are other causes for back pain can be suspect in this patient
4) Can it be TB/Malignancy
Comments
Post a Comment