This is online E-blog, to discuss our patient de-identified health data shared after taking her guardian's signed informed consent. Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input. This E-blog also reflects my patient's centred online learning portfolio. I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Following is the view of my case:
CASE:
A 61 year old male patient with chief complaints of
Shortness of breath since 1 year (grade 4)
Pedal edema since 3 months
Giddiness since 1 week
HOPI:
He was apparently asymptomatic 25 years ago and he was diagnosed to be diabetic as he had a history of loss of consciousness while he was going to washroom.
He used diabetic medication for 15 years and then he stopped medication as his blood sugar levels were normal and he also used ayurvedic medication for some days
Since 6 years he is on regular medication again.
*His Shortness of breath is aggravated on lying down and relieved on sitting position SOB is since 1 year,worsening since 1 week shifted from grade 3 to grade 4
H/O pedal edema started 2 years back ,progressively increasing and is pitting type and edema also started over hands and face since 8 months which was decreased on using medication (diuretics) intermittently edema is worse in morning time and it slightly decrease after sometime
Not associated with palpitations,chest pain,sweating,tremors
H/O CAD and severe SOB in January at 10 pm and admitted to a hospital in Hyderabad and was diagnosed to be having Myocardial infarction
In February he presented to casualty in our hospital in view of SOB grade III to IV shift
Past History:
*K/C/O type 2 diabetes since 25 years on irregular medication
*K/C/O hypertension since 15 years -was on irregular medication and using regularly since 8 years.
Personal history:
Diet- mixed
Appetite- normal
Sleep - adequate
Bowel and bladder movements: normal and regular
- alcoholic.90-180ml whiskey from 20 years of age weekly once and stopped taking alcohol and eating mutton and chicken since 10 years
as he went to yoga classes and did as they said
On examination:
Pt is conscious,coherent and cooperative.
Pallor - present
Icterus - absent
Lymphadenopathy-absent
Clubbing-absent
Cyanosis-absent
Edema-B/L pitting edema of legs:
Vitals:
Afebrile
PR : 92bpm
RR: 24 cpm
BP: 130/80 mmhg
Spo2: 84%
94% on 6 litres of oxygen
CVS:
S1,S2 heard
RS:
B/L inspiratory crepts
P/A:
soft, nontender
CNS:
Reflexes : intact
Investigations:
Ultrasound:
2D Echo:
ECG:
On 20/09/2021:
ABG:
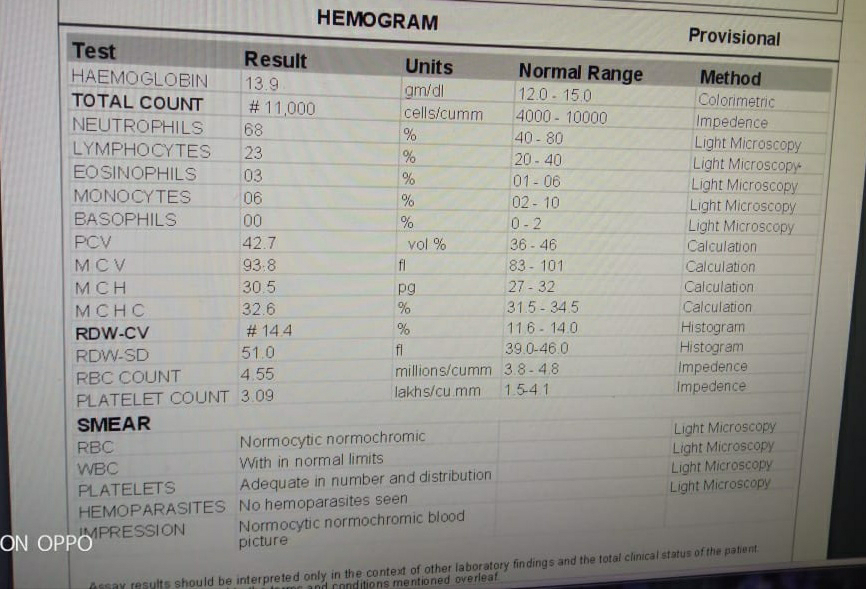
Hemogram:
CUE:
On 22/09/2021:
ABG:
Serum electrolytes:
Serum creatinine:
Blood urea:
#)
Chest X-ray:
On 20/09/2021:
On 22/09/2021:
Provisional diagnosis:
HFpEF ( EF: 52%) with chronic renal failure
TREATMENT:
1.Propped up posture
2.O2 inhalation
3.Inj Lasix 50 mg iv / tid
4.Tab . Ecospirin AV PO/ OD
5.Tab. Carvedilol 3.125 mg PO/ OD
6.Tab.pan 40 mg PO/OD
Tab. Amlong 5 mg PO/ OD
7.Tab. Vildagliptin 50 mg PO/ OD
8.Fluid restriction <2 lit / day
9.Salt restriction <2 g / day
On 20/09/2021:
On 21/09/2021:
On 22/09/2021:
On 23/09/2021:
On 24/09/2021:





















Comments
Post a Comment