50 year old male patient with weakness in right and left lower limbs and slurred speech
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient' problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
50 year old male with
weakness of both lower limbs
and slurring of speech since 5 days
History of presenting illness:
Patient had a history of fall 1 year ago and he did not take any treatment for it and was alright for 8 months then 4 months back he had pain in right hip which was insidious in onset and gradually progressive in nature
since 1month there was change in the gait of patient which was noticed by his relatives and there is hematuria for 5 days which he has neglected
For which he consulted local doctor and diagnosed avascular necrosis of of femur for which he has given medication
After taking medication he developed weakness of both lower limbs but more on right side where he could not walk , stand and eat and he need assistance for these activities
On 01/06/2022:
He had developed generalised weakness and couldnt feed himself not a/w dysphagia.
Past History:
He is a known case of Diabetes mellitus (since 12years)
Patient is using insulin two times per day.
15U before breakfast and 10U in the evening.
Not a known case of HTN,CAD,ASTHMA,TB and EPILEPSY.
Personal History:
Diet - Mixed
Appetite - Normal
Sleep - adequate
Bowel and Bladder movements - Regular
No known allergies.
Smoker - For 10 years,1-Beedi/day and paused it 4 years ago and resumed one year back.
Alcohol - For 25 years and stopped drinking when he was diagnosed with DM
He used drink continuously for 10days and stop for 20days and repeat it every month.
Family History:
Insignificant
General examination:
Patient was conscious , coherent, and cooperative well oriented to time , place person
He is moderately built and moderately nourished
Pallor- mild
icterus- absent
cyanosis- absent
clubbing- absent
Lymphadenopathy - absent
Edema- present
Vitals:
On 02/06/2022:
Bp - 120/80mmhg
PR - 92bpm
RR -17cpm
SpO2 -97%
GRBS - 150mg/dl
Not associated with fever,SOB and chest pain.
Systemic examination:
▪CVS-- s1 ,s2 heard no murmurs
• Respiratory system- normal vesicular breath sounds heard
• Abdomen- no tenderness no palpable mass , not distended
On 03/06/2022:
c/c/c and afebrile
CVS - S1 S2+
CNS - Sensorium improved
P/A - soft and non tender
stools passed 4 days back.
On 04/06/2022:
c/c/c and afebrile
BP - 120/80mmhg
PR - 88bpm
CVS - S1 S2+
CNS - Sensorium improved
R/S - BAE + and LT CREPTS +
P/A - soft and non tender.
On 05/06/2022:
c/c/c
BP - 100/60mmhg
PR - 92bpm
CVS - S1 S2+
CNS - Sensorium improved
R/S - BAE + and LT CREPTS +
P/A - soft and non tender.
On 07/06/2022:
BP - 120/80mmhg
PR - 92bpm
Atrophy of right calf region
sensations of both limbs - intact
absence of mobility of both limbs


Provisional Diagnosis:
Hypokalemic periodic paralysis
Investigations:

On 03/06/2022:
ON USG
Rt kidney - 8.8 * 4.2 cm
Lt kidney - 10*3.6 cm
Size is normal but increased echotexture
CMD - partially maintained
Spleen - 12.9cm (increased)
FINDINGS ON USG
Multiple intraductal and parenchymal calcification noted in pancreas involving and head and pancreas.
8mm calculus noted in inferior pole of left kidney.
Distended gall bladder with calcification noted of 6mm.
IMPRESSIONS ON USG
• Cholelithiasis with GB sludge
• chronic pancretitis
• left renal calculus
• mild splenomegaly
• B/L grade - II RPD changes
• minimal ascitis
On 02/06/2022:



















ECG Reports:
On 02/06/2022:

On 06/06/2022:
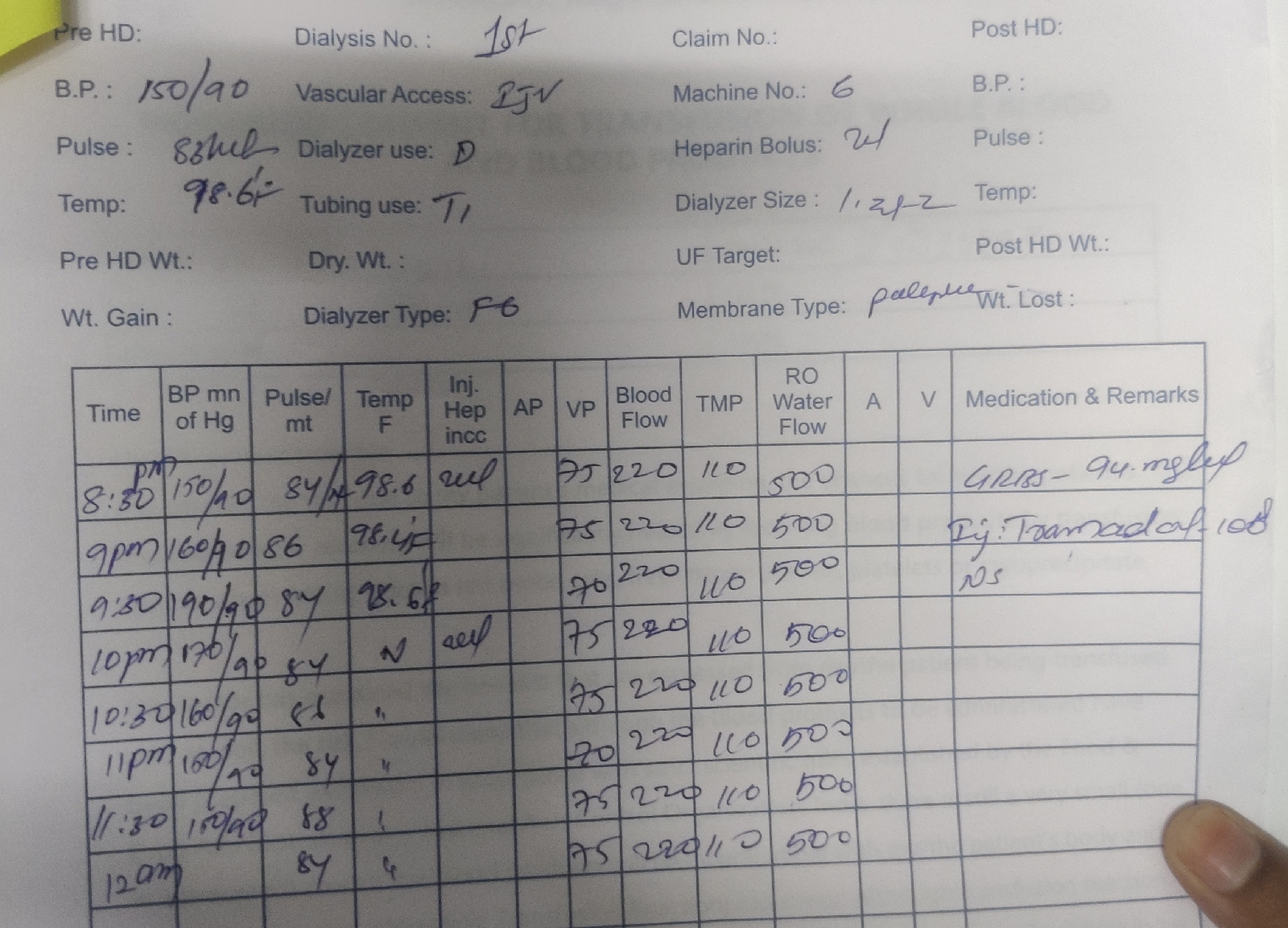
Treatment:
IVF RL NS @ 75ml/hr
Inj HAI s/C TIDaccording to sliding
Tab Azithromycin 500 mg po/ od
Tab ecosprin 75 mg PO/ OD
Tab atorvas10 mg
syp pot chlor 15 ml
syp cremaffion
Tab spironolactone25 mg
high protein diet
Tab ultraset



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment