29 year old with fever and loose stools
This is an online E logbook to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from an available global online community of experts to solve those patients clinical problems with collective current best evidence-based inputs. This e-log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box are welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient
clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Following is the view of my case :
Date of admission :29/10/22
A 29 year old male patient came to the opd with chief complaints of fever since 2 days,loose stools since 2 days
History of present illness :
Patient was apparently asymptomatic 2 days back then he developed :
H/o Fever-
Onset -
Duration- since 2 days
Type - intermittant ,high grade
It was relieving on taking medications .
Associated with chills and rigors.
Diurnal variation absent
No rise of temperature at night
H/o loose stools:
Onset - sudden
Duration- 2 days
No.of episodes -3 episodes per day
Consistency- watery
Volume -normal
Colour - yellow colour
Non foul smelling
No c/o headache,body pains,cold,cough,sob, bleeding manifestations, burning micturition.
Daily routine: Patient is a worker at a petrol station often does 24 hours shift and gets a day off
Eats breakfast at :9-10 am
Lunch at:2:30pm
Dinner at :9:00 pm
Past history:
Not a known case of,
Hypertension, diabetes, epilepsy, CAD, asthma, thyroid.
Personal history :
Diet - mixed
Appetite - normal
sleep - adequate
Bowel and Bladder movements -passing watery stools
Addictions - no
No known allergies
Drug history :
No significant drug history
Family history :
No significant family history
General examination :
Patient is conscious ,coherent ,cooperative and was well oriented to time ,place and person
at the time of examination
He is examined in a well lit room, with consent taken.
He is moderately built and well nourished.
Pallor - absent
Icterus - absent
Cyanosis - absent
Clubbing - absent
lymphadenopathy - absent
Pedal edema - absent
Vitals : on the day of admission:(29/10/2022)
Temperature - 99°F
Pulse rate - 82 bpm
Respiratory rate - 16 cpm
Blood pressure - 110/80 mm Hg
SpO2 - 99% on Room air
GRBS - 97mg/dl
Systemic examination:
CVS :
S1 and S2 heart sounds heard
NO murmurs and thrill
RESPIRATORY SYSTEM :
Bilateral air entry present
position of trachea - central
Vesicular breathsounds heard
CNS : intact
ABDOMEN:
Soft,nontender
On deep palpation: no palpable mass
No organomegaly
Bowel sounds heard
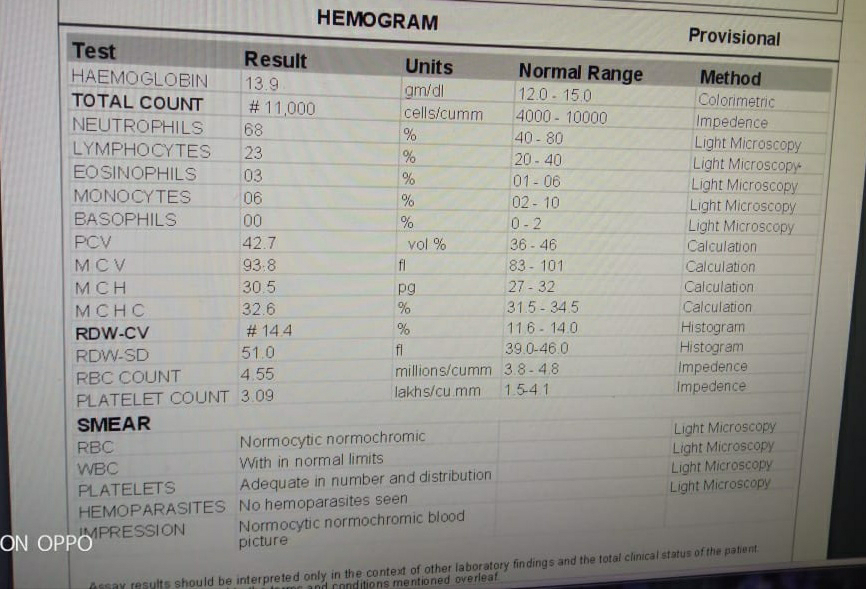
Investigations:











Diagnosis:
Dengue with Bicytopenia(WBC,PLATLETS)
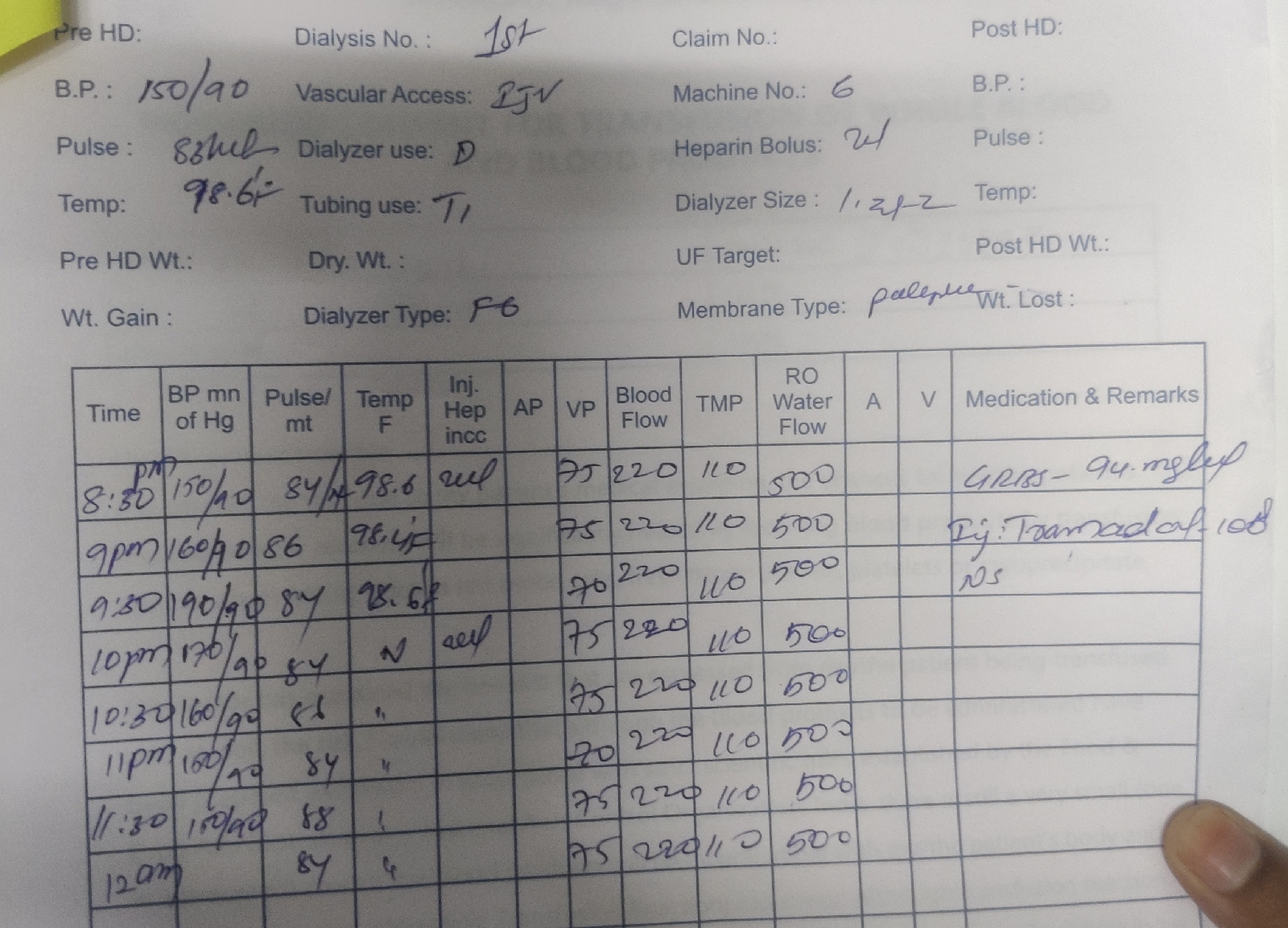
Treatment:
1)IV fluids : 2*NS 1*RL
2)plenty oral fluids
3)strict temperature charting 4 th hourly
4)T.Dolo 650 mg /PO/SOS
5)Inj.Neomol 1gm IV SOS(if temp >101°F)
6)Tab.Pan 40 mg PO/OD
7)W/F bleeding manifestations,postural hypotension
Comments
Post a Comment