This is an online E logbook to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from an available global online community of experts to solve those patients clinical problems with collective current best evidence-based inputs. This e-log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box are welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient
clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Following is the view of my case :
Date of admission :5-11-2022
Chief complaints :
C/O
A 62F,farmer by occupation came with
Weakness since 2 days and tingling sensation in left lower and upper limbs since 1 week
HOPI:
Patient was asymptomatic 1 week ago (till last sunday)and going to her work till sunday,and stopped working since sunday as she developed tingling of left upper limb and lower limbs and when she was about to wakeup in the early morning (4:00 am)for washroom,she was unable to get up from the bed and noticed weakness of left sided upper and lower limbs associated with tingling sensation,the very next day local RMP doctor noticed high recordings of BP and gave her anti hypertensives and advised her to higher centre and she came to OPD yesterday.
No c/o fever,vomitings,loose stools,giddiness
No c/o slurring of speech,and no drooling of saliva.
No c/o chestpain,palpitations,syncopal attacks.
Past history:
Not a k/c/o HTN,DM,TB,ASTHMA,CAD,EPILEPSY
Personal history:
Diet - mixed
Appetite - normal
sleep - adequate
Bowel and Bladder movements -regular
No known allergies
Addictions:Tobacco smoker since 40years
Alcoholic since 40years,(90ml)once in every 10days
Family History:
Not Significant
Drug history :
No significant drug history
General examination :
Patient is conscious ,coherent ,cooperative and was well oriented to time ,place and person
at the time of examination
SHe is examined in a well lit room, with consent taken.
SHe is moderately built and well nourished.
Pallor - absent
Icterus - absent
Cyanosis - absent
Clubbing - absent
lymphadenopathy - absent
Pedal edema - absent
Vitals at admission:
Pt is c/c/c
Bp:130/80mmHg
PR:88bpm
Cvs:s1 and S2 heard
RS: NVBS,BAE PRESENT
P/A:SOFT,NON TENDER
CNS: HMF intact
Motor system examination
Tone
Rt. Lt
UL. N. Decreased
LL. N. Decreased
Power
Rt. Lt
UL. 4/5. 0/5
LL. 4/5. 3/5
Reflexes
B. T. S. K. Ankle
R. ++ ++ ++. ++. -
L. - - - - -
R plantar flexor
L plantar extensor
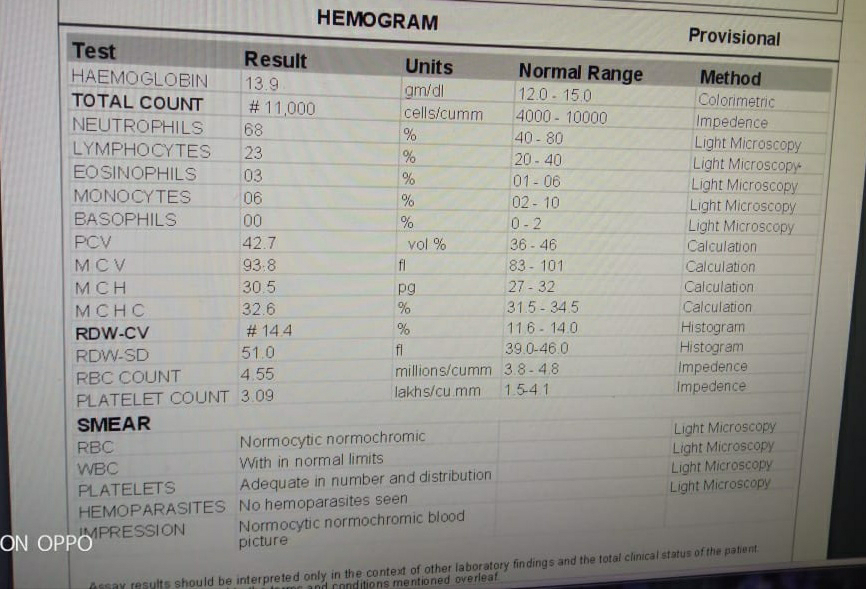
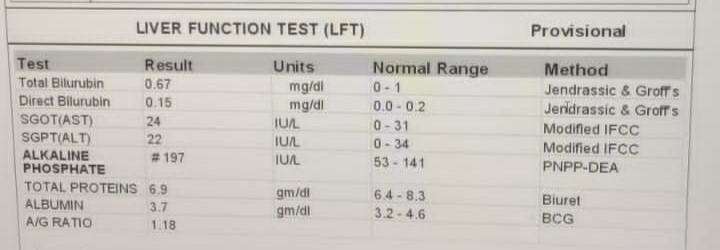
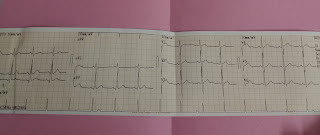
Investigations:
DIAGNOSIS:
Acute infarct in right occipital lobe,right posteriotemporal lobe and right thalamus- PCA TERRITORY
Treatment:
T.Ecospirin 150mg po od
T.clopitab 75 mg po od
T.atorvas 20 mg po od
T.pregaba M 75mg po od
Vitals monitoring 4th hrly









Comments
Post a Comment